Search Podcasts

Listen in as Dr. Mike provides the answers to a wealth of health and wellness questions.
Additional Info
- Segment Number 5
- Audio File healthy_talk/1522ht2e.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 26, 2015
You're listening to RadioMD. It's time to ask Dr. Mike on Healthy Talk. Call or email to ask your questions now. Email: AskDrMikeSmith@RadioMD.com or call 877.711.5211. The lines are open.
DR MIKE: So, continuing with our conversation about wound healing, I have a question about a dog bite. It's really not about the dog bite.
"I'm recovering from a dog bite. There's no rabies, just a slow healing wound. I read that certain amino acids are critical to wound healing. Can you please review some of these?"
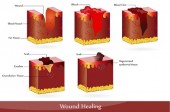
Yes, so this is a continuation from the previous discussion about wound healing where I talked about calories and making collagen and cell proliferation. I talked about carbs, protein fat, vitamin C, zinc, B vitamins, water --all those are important to any wound. It doesn't matter what caused the wound. But this person is specifically asking about certain amino acids that play a role in wound healing.
I had to do some research here. I was more familiar with more the general nutritional suggestions for wound healing but when it came to amino acids, I did some research and found some interesting stuff. And what I discovered--let me go ahead and --there's two amino acids that are really important.
But then, just doing this research, I discovered some other things like bromelains and glucosamine, aloe vera, curcumin. So, let me just kind of first start with amino acids but then I want to share with you some of the other information that I found when I was researching the amino acids.
So, the first amino acid that seems to be really important to any wound is arginine. I think most of you are familiar -- you know we use arginine, traditionally speaking, for nitric oxide production, cardiovascular system, erectile dysfunction for men, that kind of stuff. There's even a link to testosterone. But arginine also - besides all of that more traditional use - arginine is important to a part of the immune system called the cellular immune response. And it's the cellular immune response that fights bacterial infection.
And, as you know, in open wounds that's critical. Often one of the reasons a wound, especially from a bite -- human, dog, cat, doesn't really matter -- is the introduction of pathogenic bacteria and you get this smoldering ongoing infection that's really hard to treat in many cases. And that leads to this chronic wound that never really closes up. Maybe it does eventually close up. It could take months, even years down the line but now you have a nice scar.
Turns out arginine could really help in this process. It says here, I got this from some research coming out of-- let's see this was the Journal of Nutrition from a Dr. Patel in 2005--he was looking at arginine and found that it was not only important to the cellular immune response but it was also important to protein synthesis at the wound site and increases local wound immune function. He was recommending 17 to 25 grams of oral arginine a day and that's in contrast to the normal daily requirement of 5 grams. So, you're talking about a substantial increase in the amount of arginine for a chronic wound.
And again, it's fighting the bacteria and, according to Dr. Patel, it's also increasing protein synthesis at the wound site.
The second amino acid was glutamine. Glutamine is just critical for fast growing and multiplying cells along with B vitamins; along with zinc. I mentioned those before but in this case, just focusing on the glutamine. Glutamine probably has its largest effect, its greatest effect, I should say, on the proliferation of fibroblasts which are these cells that are important to your eating up the necrotic tissue and laying down brand new connective tissue.
So, fibroblasts play an important role in the closure of a wound. Glutamine has a great impact on those fibroblasts. As a matter of fact, there was, in my research, I came across a couple of pathology books that talked about how during the creation of a wound and in a few weeks after that wound was created, glutamine is one of the major amino acids that is lost during that tissue injury.
I thought that was pretty interesting. They didn't really explain why, but glutamine is depleted during tissue injury. So, that really implies a significant role, obviously, in wound repair. We've got to get that glutamine back into your system. According to researchers, glutamine possesses anabolic properties. That's building-up properties which are effective in wound healing.
But you need amounts about two to seven times greater than required in healthy persons and that came from a Dr. Roth in 1990. So they've been looking at glutamine for quite some time now in wound healing. But you've got to do a lot - two to seven times more than what a healthy person might need.
Now, what about some of these other...So those are the two amino acids--arginine and glutamine--for wound healing. But in this research, as I said, I came across some other pretty interesting stuff. Bromelain from pineapple, some proteolytic enzyme, and I've heard about bromelain's healing properties before.
I even know some plastic surgeons that use bromelain to close up wounds, surgical wounds. It just has strong anti-inflammatory properties and is able to break down and dissolve proteins that need to be broken down in the wound so that you can rebuild that connective tissue. There is even a study showing that bromelain led to a faster resolution of swelling and a decreased dependence on pain medications.
Now in that particular study, it was looking at patients with open wounds from fractures. Those can be horrific open wounds, you know? Bromelain was beneficial in those really horrific type injuries. So, that's very promising. That's bromelain. Now, if you eat pineapple you'll get a little bit of bromelain. It does break down protein, as we said. As a matter of fact, you can use pineapple and stuff like that, papaya, as meat tenderizers, because there's bromelain in there and it breaks down the protein. But you're not going to get enough.
You are going to have to look for bromelain supplement. Glucosamine is very important. I think most of my listeners, you guys are familiar with glucosamine as a joint product, right? Glucosamine, MSM, chondroitin, although I don't use chondroitin. It's too big of a molecule. It doesn't absorb well. But glucosamine is classic for joint health, joint repair. And yes, it's great for wound healing as well. It repairs connective tissue. It repairs skin, tendons, ligaments, joints. Animal studies show that levels of glucosamine increase in injured tissue during healing. So, the body knows it's important so when someone is trying to heal, you can measure a certain amount of glucosamine in the healing tissue.
Now, the human studies, when I was doing my research, the human studies on the effects of glucosamine in wound healing really weren't there yet. There's a lot of cell culture studies. There are some studies identifying the fact that glucosamine is in a healing wound, like I mentioned, but there's not a lot out there about the ability of glucosamine to actually heal, to repair, to regenerate and close up the wound.
So, it's hard for me to even give you a dose on this. But I would, probably, if you want to try glucosamine, you're probably going to want to maybe double what you might normally find in a joint product -- so 1500mg, 2000mg, maybe even 2500mg of glucosamine.
Aloe vera has some healing properties, so that's something else you might want to try. An animal study showed that it's helpful in frostbite, electrical injuries, diabetes. And then, of course, one of my favorites, curcumin, is a great anti-inflammatory. So, there are some suggestions but to answer the question, arginine and glutamine -- good amino acids for healing.
This is Healthy Talk on Radio MD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD
Listen in as Dr. Mike provides the answers to a wealth of health and wellness questions.
Additional Info
- Segment Number 4
- Audio File healthy_talk/1522ht2d.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 26, 2015
It's time for you to be part of the show. Email or call with questions for Dr. Mike now. Email AskDrMikeSmith@RadioMD.com or call 877.711.5211. What are you waiting for? The doctor is in.
DR MIKE: So, my first question is about a non-healing wound. It most commonly occurs in people who are immunosuppressed, diabetics--really anybody with a chronic disease often has issues with healing. And when I mean wound, this could -- you know, I have this question here from a listener. I don't know he or she.
I don't have a name. Doesn't even tell me what caused the wound. But when we say "wound", it could be a surgical wound -- you know, on purpose. Somebody went in and cut you open to, I don't know pull, out a tumor or infection, whatever. Or, it could be from an accident or trauma.
So, I'm using wound very generally here. But it doesn't, at the end of the day, there's a break in the skin and the body is supposed to be able to heal that, repair that and regenerate healthy tissue.
And for whatever reason -- again in those people with chronic diseases, immunosuppression, they often have a hard time in that healing process and it just doesn't work right. Sometimes it even overdoes it. You ever heard of a keloid? That's one of the scars that really kind of builds up and it's very visible. That's called a keloid. It happens in African-Americans more than anybody else for some reason. We still don't understand. So, sometimes you can get the reverse. You get this hyper healing. Let me just get to the question here.
"I have a wound that won't heal. I don't have diabetes. I write that because that's the first thing people ask. What should I be taking or not taking, to speed up healing?"
Now I'm going to keep to the question here. So, this person is asking taking something, right? So, either medicine, supplements – again, it's not about applying anything but about taking. I'm assuming something like a pill and that's what they are looking for.
And I'm going to stay away from the pharmaceutical stuff and I'm going to focus more on what we can do over the counter. Some basic things that maybe this person or, if you're somebody who has a wound that's not healing properly, it's taking a long time. Diabetic or not, immunosuppressed or not, these are some things that definitely can help with wound healing.
And the first thing -- you know there's a lot here -- let me do this, let me just read off probably the most important things and then I'll get into the specifics as much as I can. So, let me just read off the most important things to wound healing. Number one: calories. I'll get to what that means but you got to eat. Calories are important. Carbohydrates are important.
Protein, fats, vitamin A, vitamin C, zinc, and water. So, let's talk about each one of those individually. Calories: it takes a lot of energy to heal a wound. The larger the wound the more calories you need, right? You have to maintain sufficient energy supplies to have a robust immune response that can bring in the reparative cells. You have to have an energy supply that can produce the reparative hormones, like growth hormones in the insulin, like growth factors that are involved in wound healing.
Often what you see, especially if the wound is large and the person maybe even has an infection from it, obviously that infection has to be treated.
But the larger the wound the less active the person is, the less they feel like eating, especially if they are older. That can be bad and detrimental but we need to make sure that we're getting enough calories to supply this reparative process. There was a study published by a doctor named Leininger in 2002.
I don't have the journal here but Dr. Leininger is really one of the world's leaders in chronic wound healing and he has estimated that especially in older people you might need an increase of up to 25 to 30 calories per kilogram of weight. That's a lot! That's a lot of calories. So, yes, we have to make sure that we're eating enough to supply that reparative process. Carbohydrates are important to wound healing.
Carbohydrates have been shown to help meet the body's heightened energy requirements. That's number one. Number two, they aid in fibroblast movement which is vital in wound healing. A fibroblast is a type of cell that can come in there and eat up some of that necrotic decaying material, help to lay down some new connective tissue for the reparative process, and carbohydrates are important to enhanced white blood cell activity to strengthen your immune system. So, make sure you're getting a nice rich source of complex carbohydrates. Protein--very important and necessary for collagen synthesis. You know, collagen is the main connective tissue.
I mean, there's other connective tissue proteins but collagen is the key one and we have to make sure that we are taking in enough protein to do the normal things protein does. But at the same time increase collagen synthesis for the wound healing process. Along with collagen there would be one of the vitamins that I mentioned here and that is vitamin C.
So, you want to increase your protein intake for collagen. but then you also want to make sure you're getting vitamin C, maybe a 1000 to 2000 milligrams a day.
That's far above the recommended daily intake by the way, which is only about, I don't know, 50 to 100 milligrams. Vitamin C plays an important role in helping the body generate collagen, so as you're taking in more protein you need the vitamin C to activate an enzyme called procollagen hydroxylase.
Procollagen hydroxylase is the enzyme that helps to bring these parts of collagen together to actually make it strong. So, we want to increase calories; we want to make sure we're getting our carbs. We've got to bring in our proteins for collagen synthesis and then we got to make sure that we have enough vitamin C on board to activate that enzyme that makes the collagen as well. Fats play an important role, too.
The essential fats, phospholipid based fats, phosphoryl choline based fats are very important because those aid in the cell membrane and cell structure of the new cells that are being laid down in the wound. So, fats are very important. Zinc. You know, some research looking at zinc in wound healing has been very positive. Zinc plays an important role and I might go ahead and add to this B vitamins as well. So, zinc and B vitamins, they play important roles in cell proliferation and cell regeneration.
So, zinc and B vitamins: if you're eating enough calories, you're bringing your carbs, your fats, your proteins, you got enough vitamin C on board. So, you're producing more collagen and all that kind of stuff. But if you're not aiding in the regeneration of healthy cells which make healthy tissues, the whole process could break down and that wound can take a long time to close up. So, zinc and B vitamins play an important role in cell division and cell proliferation in the closing up of that wound.
And then don't forget about water. You know, when you're trying to repair a wound the larger -- this is even more true -- you're almost in a hyper metabolic state and that can leave your body what we call volume depleted. I don't like to use the word "dehydrated" because if you're dehydrated, you'd be dead. Dehydrated is without water. You'd be like a prune. So, I call it "volume depleted". But when you're hyper metabolic, you're activating all of these cell proliferation pathways, collagen production pathways, immune pathways, you're using a lot of water up, so make sure to remain hydrated.
So, calories, carbs--complex carbs--protein for collagen synthesis, fats for cell membrane structure and function, vitamin C for the collagen production along with the protein, zinc and B vitamins for cell proliferation and closing up that wound, and water for the hyper metabolic state. All of those might be helpful in wound healing.
This is Healthy Talk on Radio MD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

Why is preventing C. diff (clostridium difficile) important?
Additional Info
- Segment Number 3
- Audio File healthy_talk/1522ht2c.mp3
- Featured Speaker Stephen J. Schrantz, Jr., MD, MA
- Organization C. Diffense
-
Guest Bio
 Dr. Stephen J. Schrantz is a board-certified infectious disease physician at NorthShore University HealthSystem. He is also a Clinical Assistant Professor at the University of Chicago Pritzker School of Medicine. Dr. Schrantz received his medical degree from The Chicago Medical School. After completing his residency training in internal medicine and pediatrics at the University of Chicago, he went on to complete a fellowship in infectious disease at the same institution.
Dr. Stephen J. Schrantz is a board-certified infectious disease physician at NorthShore University HealthSystem. He is also a Clinical Assistant Professor at the University of Chicago Pritzker School of Medicine. Dr. Schrantz received his medical degree from The Chicago Medical School. After completing his residency training in internal medicine and pediatrics at the University of Chicago, he went on to complete a fellowship in infectious disease at the same institution.
His clinical interests include: illness in returning travelers, infection associated with healthcare contact, infections associated with implanted devices, new diagnosis HIV or ongoing care, bone and joint infection, fever of unknown origin, skin and soft tissue infection, and prevention of infection.
He has co-authored many articles pertaining to infectious disease and has been featured on the Chicago news stations, WGN-9, ABC-7, and CBS-2, for his medical expertise. -
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 26, 2015
Anti-Aging and Disease Prevention Radio is right here on Radio MD. Here's author, blogger, lecturer and National Medical Media Personality Dr. Michael Smith, M.D. with Healthy Talk.
DR. MIKE: So, let's continue our discussion about C. diff and get into more the prevention of C. diff, which is really going to be the key. Just as a quick review, C. difficile is a bacterial infection. It happens mostly in hospitalized patients who have been on antibiotics and certain procedures. It causes horrific diarrhea and, of course, this is happening in people that are already sick. That's why it can be so devastating.
So, really, prevention is the key. I'm here with Dr. Steven J. Schrantz. He's a Board Certified Infectious Disease Specialist out in Chicago. He's just been all over the media talking about some of the research he's doing in C. diff.
Dr. Schrantz, welcome to Healthy Talk.
DR. SCHRANTZ: Thanks.
DR. MIKE: I went online and researched in Google and I put "fecal transplant" in. I found that there's a Fecal Transplant Foundation. There's people doing in-home fecal transplants for different things. Why don't you explain what you're doing with this as far as treatment for C. diff?
DR. SCHRANTZ: Sure. My colleagues and myself are looking at fecal material transplantation to mostly treat recurrent C. diff. The way we've proceduralized it is to either give it via colonoscopy or to give it by a quick enema at the bedside. Both have shown to be effective. That's one of the things that we are looking at – what's the best way to do this?
Things are really quickly growing in this field. Now companies have been established that are developing products that are mimicking stool or are stool themselves that people are starting to look at in the home to treat recurrent C. diff. The other interesting area is could we be using this technology - technology sounds like a funny word to use for a stool transplant - we are doing that now earlier for treatment rather than just for recurrent. So, we are starting to look at that.
DR. MIKE: But what does it really do? What is the mechanism of action when you transplant the fecal material into a patient? What's going on there?
DR. SCHRANTZ: I think the easiest way to think about it is that we are re-establishing a balance of bacteria in your colon. As we are learning more and more about the body, this is one of the areas that we didn't understand that much about. Now we are beginning to realize that there are over 5000 different species of bacteria in the colon and they are all working together to provide us nutrients and prevent disease. When a lot of them are taken away by the use of antibiotics, we need to think about re-establishing that healthy bacteria in our colon. And that's exactly what we do. We take healthy bacteria from one person and give it to another.
DR. MIKE: The difference between the fecal transplantation and just a probiotic product is the number of healthy bacteria--the number of healthy species, correct? A probiotic might have anywhere between one to seven species but here you are taking just what's naturally in someone's colon. You are getting a balance of all these healthy probiotics. So, that's an interesting treatment. And you're having some success with this initially, right?
DR. SCHRANTZ: Yes, so studies have been done at our institution but also elsewhere and have shown that this is a very effective treatment for C. diff. I don't want to get into it too much, but people are really starting to think about how else we can look at this. What other diseases are being impacted our fecal microbiota?
DR. MIKE: Let's bring this back to C. diff. Dr. Schrantz, when you talk about treatment, you talk about fecal transplant, you talked about enema, colonoscopy. These are all words that people don't like to hear. So, at the end of the day, prevention is obviously going to be a lot easier. What are we doing in the field of C. diff prevention that you think looks really exciting right now?
DR. SCHRANTZ: In the past, all we've had is making sure people wash their hands and trying to limit the amount of antibiotics that people get exposed to. But now we are starting to think even more about how we can robustly prevent C. diff. One of the products that is being invented and being currently studied is a new vaccine product.
We all know vaccines are a fantastic way to prevent disease. Measles, mumps. One of the things that we all get vaccinated for routinely is tetanus. tetanus is Clostridium Tetani, the bacteria that causes that infection. It produces a toxin and it's the toxin that produces tetanus. The way the vaccine is generated there is they take the toxin and they denature it and they give it to you with the hope that your body gives an immune response to that toxin. So, if it ever sees it again, it recognizes it.
We've taken that same idea and we've applied it to its biologic relative, if you will, Clostridium Difficile. There's now a vaccine that's going to stimulate your body's immune response to the toxin. So, if you ever see it, you don't get the disease. This is an ongoing trial. A Phase III trial they say. There are over 200 sites word-wide that are looking at this and we happen to be one of them. We are looking for 15,000 healthy people who are at risk for C. diff to help us understand whether or not this is going to be an effective treatment.
DR. MIKE: Do you see this vaccine being used in the community or is it really just for people who are coming into the hospital and they get the vaccine? Like that's part of their workup now.
DR. SCHRANTZ: I think that's a fantastic question. I think it's hard to know at this time where the best place to use the vaccine is going to be. I can see it easily being used preventatively in patients that are going to be at risk.
We will be able to establish some known risk factors and once we establish those we say, "Okay. You are going to need the vaccine", rather than giving to infants at birth. I don't think it's at that stage. It is certainly something we can target people who are at risk and give them a vaccine that would prevent a serious complication to the hospitalization that might be coming up or that they might be at risk for.
DR. MIKE: Who's eligible for your study?
DR. SCHRANTZ: We are looking at two groups. The first group is people who are over the age of 50, that have been in the hospital at least twice during the last year and have had some antibiotics. The second group of people are people who are planning a major surgical procedure that is going to land them in the hospital for at least three days after the procedure.
Both of those groups are people who are at risk for C. diff. Anybody who has had C. diff, unfortunately, is not eligible for the study. What's unfortunate about it is that those are the people that really know they don't want to get it. So, we are trying to get the word out to let people know that this is a real problem, this is a growing problem and this is something that we are really working hard to find a good preventative strategy to help people stay healthy.
DR. MIKE: You mentioned that this is in Phase III. So, for my listeners this is kind of pre-market research looking for that approval. What is the timeline? If Phase III pans out and you get the results you want, what are we looking at? A year down the line? Two years? Three years?
DR. SCHRANTZ:I think we are looking at two to three years down the line at this point but that's not up to me. I'm just helping out with the study the best I can. The hope is sooner rather than later. I really think this could help a lot of patients.
DR. MIKE: If my listeners are interested in this, where can they go to find out more about this study? Is there a number or a website?
DR. SCHRANTZ: The website people can go to if they are interested in a study is: www.cdiffense.org and if you are in the Chicagoland area you can call us at: 847-570-3558. We can get in touch with you regarding whether or not you'd be able to participate in the study.
DR. MIKE: Well, Dr. Schrantz, we are going to have to leave it there. Thanks for coming on. Awesome work. Please continue what you're doing because we know that this is serious. It's nice to see that we may have a decent prevention down the line. This is Healthy Talk on Radio MD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

C. diff (clostridium difficile) commonly affects older patients in the hospitals or those placed in long-term care facilities like a nursing home.
Additional Info
- Segment Number 2
- Audio File healthy_talk/1522ht2b.mp3
- Featured Speaker Stephen J. Schrantz, Jr., MD, MA
- Organization C. Diffense
-
Guest Bio
Dr. Stephen J. Schrantz is a board-certified infectious disease physician at NorthShore University HealthSystem. He is also a Clinical Assistant Professor at the University of Chicago Pritzker School of Medicine. Dr. Schrantz received his medical degree from The Chicago Medical School. After completing his residency training in internal medicine and pediatrics at the University of Chicago, he went on to complete a fellowship in infectious disease at the same institution.
His clinical interests include: illness in returning travelers, infection associated with healthcare contact, infections associated with implanted devices, new diagnosis HIV or ongoing care, bone and joint infection, fever of unknown origin, skin and soft tissue infection, and prevention of infection.
He has co-authored many articles pertaining to infectious disease and has been featured on the Chicago news stations, WGN-9, ABC-7, and CBS-2, for his medical expertise. -
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 26, 2015
Living longer and staying healthier. It's Healthy Talk with Dr. Michael Smith, MD. Here's your host, Dr. Mike.
DR MIKE: So, why am I talking about something called C. diff and why am I worried that you might be at risk for it and why did I bring on a guest who is an expert on C. diff? His name is Dr. Steven J. Schrantz. He's a board certified infectious disease physician at North Shore University Health System. He is also a clinical assistant professor at the University of Chicago. He's co-authored many articles pertaining to infectious disease and has been featured on the Chicago news stations--all the big ones like WGN9, ABC7 for his medical expertise.
Dr. Schrantz, welcome to Healthy Talk.
DR SCHRANTZ: Thanks for having me.
DR MIKE: Why don't we just start out with what is C. diff and why am I having you come on talking about this?
DR SCHRANTZ: C. diff is one of those infections probably many of your listeners have not heard of. C. diff is short for clostridium difficile which is a bacteria that can create a horrible diarrhea and I know nobody likes to talk about diarrhea, but we all know it can be absolutely horrible and this is the worst of them. It's generally acquired in the hospital, so most of the patients that we have that are infected acquired it in addition to some other problem that brought them into the hospital in the first place. Unfortunately, this can make patients extremely ill.
Only about one-third of them are actually acquired out in the communities, so this is mostly a hospital problem. With that being said, they're some of the sickest patients in the hospital already and then this, unfortunately, can be a complication that can lead to death. It's a serious bacteria that secretes a toxin and it's the toxin actually that generates the inflammation in the colon that leads to the diarrhea and that's become a big problem. The current numbers on that, there was just a New England Journal article that was published in April that suggested 453,000 cases in 2011 and that lead to about 29,000 deaths.
DR MIKE: Is that a significant increase from past years?
DR SCHRANTZ: Yes, it has been on the rise and it's been on the rise with each year. Since I've been in practice over of the last 15 years, I've seen it increase every year since then. So, since around the beginning of the decade, the beginning of the millennium, we've been noticing more and more cases and they're getting to be more and more of a problem and we're doing more and more in the hospital to try and help our patients.
DR MIKE: So, describe for me, Dr. Schrantz the type of patients in the hospital that's more at risk for this. Is this somebody's that's going through certain procedures or is just any hospitalized person is at risk? Who's really at risk here?
DR SCHRANTZ: We've identified multiple risk factors for patients that may get C. diff infection. The number one would be being exposed to some antibiotics. What happens is, we give antibiotics for all sorts of infections and, unfortunately, some things that are not infections. It's this overuse of antibiotics that has led to this. What happens is, the intestines kind of clean out all the good bacteria inadvertently by treating the bad bacteria that you're fighting with the infection and that kind of sets up a space for this new infection, this clostridium difficile to take root.
Then, once that's there, it secretes the toxin, as I mentioned, and that leads to the diarrhea. So, antibiotic use is number one. The second thing that leads to risk in the hospital is being exposed to the bacteria and that's what we're trying really hard to contain in the hospitals. We'll isolate patients and we'll make people wear gowns to go in the room to try to prevent it from spreading around the hospital. However, as you can imagine, these are bacteria and it's kind of hard to take every last one of them out.
Then, the third thing would be general kind of patient conditions--things that most of our patients don't have any control over and those are the elderly, the ones that have already had some inflammatory bowel disease, the ones that are immunocompromised due to their chemotherapy or treatment for some other autoimmune condition, organ transplant.
So, any time your immune system's down, you're going to be at more risk. The other thing would be if you have chronic kidney disease. These are things we know suppress the immune system and can lead to, vulnerability to another infection like C. diff. The third one would be something that's very common and that would be the use of acid suppressing medication. So, a lot of people are on medication to suppress the acid in their stomach and some studies have shown that can actually lead to this as well.
DR MIKE: So, are hospitals experimenting in researching the use of, say, probiotics for hospitalized patients, vitamin D, kind of some of the classic immune support nutrients? Anything going on there?
DR SCHRANTZ: Yes. So, probiotics have been looked at fairly extensively and, unfortunately, it's kind of been a mixed bag. Some studies have shown that probiotics can help prevent the infection more in the outpatient setting. Some of the studies that were done in the inpatient settings show not such a great result, but part of that is that, as you know, probiotics are kind of a new area. We're still trying to figure out which are the good bacteria, which ones do we really need and those have been challenges for the study to know whether or not probiotics works. So, I would say at this point, it's a mixed bag. I usually tell my patients, try some probiotics. It's certainly not going to hurt you and they could help.
DR MIKE: Right, right. Yes. Yes and there's also some--and I don't have the research at the top of my head, Dr. Schrantz-- but there were a couple of studies looking at healthy yeast species, not the classic healthy bacteria as a probiotic but certain yeast, certain saccharomyces yeast species, for instance, and I wonder if there's been any...Do you know if there's been any good results there?
DR SCHRANTZ: I don't know anything more about new yeast studies. Certainly, saccharomyces is the one that we see most commonly used in probiotic products so that's been the one that's been most looked at. But again, I tell patients, your colon has over 5,000 different species of bacteria and yeast and when we take a probiotic, we're really just replacing one or two of them, so I think there's a long stretch for us to go in this but I have a lot of hope for the future in that field.
DR MIKE: We do want to see more research in probiotics. What about something as simple as vitamin D and its ability to boost the immune system? Anything, any research there that may help some people?
DR SCHRANTZ: Certainly, vitamin D is something that's been linked to immune health. With that being said, there isn't anything robustly studied and it's certainly not in the setting of C. diff. We know that many of our patients living in these cold winters up here in Chicago are going to be vitamin D deficient, but it's true link to see C. diff as poorly understood.
DR MIKE: Well, I want to in the next ten minute segment, I want to talk more about preventing C. diff. Obviously, it's always easier not to get something. That's the easiest thing to do. But, in the meantime, what do we do for treatment? Are we starting to see C. diff resistance to antibiotics? How do we treat C. diff?
DR SCHRANTZ: Thankfully, we're not seeing a lot of resistance to antibiotics. We have a few antibiotics that work quite well at eradicating C. diff. When patients are initially infected, they will take a new antibiotic and the problem is about twenty percent of patients are going to have a recurrence, so we'll take care of it for a little bit and then it's going to come back and we think that's mostly due to a weakened immune system and some of the things we're doing now, and actually we're doing at our institution is, I don't know if your listeners have heard of this, but we're doing what's called fecal material transplantation now. That's where you actually take stool from a donor individual and transplant it into the colon of an affected individual with the hope of reestablishing that normal bacteria in their colon. That's kind of the new thing.
DR MIKE: You're seeing some good results with this initially?
DR SCHRANTZ:Yes. We've seen some excellent results with this. Now, that being said, we're using it just for the returns and the worst of the worst kind of case, but we are starting to experiment and think about how can we move this further into the chain because we have seen such good success with it.
DR MIKE: Dr. Schrantz, real quickly, is there a number you can give my listeners if they're interesting in looking at this study?
DR SCHRANTZ: That's one study. The other study for prevention that we're looking at is the study I'm helping them with the most which is a new vaccine product to prevent C. diff and this new vaccine-
DR MIKE: I'll tell you what, hold on to that, when we come back, let's get into that new vaccine and the importance of prevention and we can give out that number.
This is Healthy Talk on RadioMD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

Listen in to hear the latest research on AMPK.
Additional Info
- Segment Number 1
- Audio File healthy_talk/1522ht2a.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 26, 2015
Living longer and staying healthier. It's Healthy Talk with Dr. Michael Smith, MD. Here's your host, Dr. Mike.
Dr. Mike: Are natural AMPK activators the new Metformin? Now, I guess we need to discuss some parts of this question before we answer it. You might be wondering what is AMPK? You might be wondering what is Metformin? Those are good questions.
Well, Metformin is a commonly prescribed diabetic drug. It's a prescription drug for Type 2 diabetes. It's a good drug. It does--it works well, brings down blood sugar, but it's a chemical drug. It definitely has some side effects to it and any time we can find things in nature that are more natural that can do the same thing, I think that's better. If I can find something in nature that does the same thing as Metformin but without the side effects; that's just a win-win.
Now Metformin, as a prescription drug, when you take it, it's mechanism of action--what we refer to in pharmacology, the pharmacological dynamics, just a fancy way of saying what it does-- it activates an enzyme in the body called AMPK, adenosine monophosphate-activated protein kinase. This is an enzyme inside the cell.
This is not a digestive enzyme, it's an enzyme inside the cell and it's a sensor or a switch that helps to turn on and off energy pathways. When AMPK is activated, you tend to switch on pathways that generate energy and turn off pathways that consume energy. So, we see things like fat and sugar levels. All those go down because we're not generating them, we're metabolizing them when you're activating AMPK and that's what Metformin does and that's why it's so successful. It's an AMPK activator. What we have discovered now, is a couple of plant extracts that do the same thing as Metformin and without side effects.
Now, I was explaining this to a friend of mine. I do review some of my segments with some friends here and there just to see what they think, or are they following me, that type of stuff. And she said, she asked me a really interesting question and I wasn't expecting it, but it's a great question and I think we need to discuss it.
Well, if Metformin is an AMPK activator and these two plant extracts, that I'm going to describe in a second, are also AMPK activators, so how come Metformin has side effects and these two plant extracts don't? That's a great question and this, I think the simple answer, or the straight forward answer is, well, Metformin is a chemical. It's unnatural.
Now, in some cases, many of our drugs are based on natural compounds found in plants, but then the pharmaceutical companies will change them just a little bit, maybe to get better absorption, greater effect, what have you and now it's an unnatural thing. Maybe the backbone, if you will, of the drug started with a plant but they changed it enough to where's it unnatural now.
Of course, now they can patent it, make money off of it, but once it's becomes changed and unnatural, it's just harder for the body to recognize it and metabolize it so you get more side effects with it. Natural things--plant extracts, antioxidants, essential oils, all that kind of stuff--your body just knows how to deal with those. The body knows which pathways to throw these natural compounds down so you can metabolize them better.
So, yes, natural things often have less or even no side effects. So, what are these, before I go into a couple of these plant extracts and I do think the research is there to support these as the new Metformin, I really do, I'm not saying to stop your Metformin and go to these plant extracts. I'm just going to present the data to you and maybe you go talk to your own doctor about it, but the data is pretty interesting and pretty powerful. Why does AMPK, which is the cellular enzyme, why does it decrease in activity as you get older?
Well, like everything, our bodies just don't function as well; we don't produce hormones as well; we don't produce these enzymes as well; we don't activate things as well. So, the aging process itself decreases AMPK activation. We also know that overeating does, too. In America, we are-- what's that phrase? Overfed, undernourished. Right?
We're eating lots of empty calories that will decrease AMPK activation which means you're not going to manage energy better and the cells become engorged with fat, for instance, and sugar. Chronic inflammation can also lower AMPK activation. There are natural ways to boost it without taking anything: rigorous exercise, calorie restriction, all of that stuff will help, but you're not going to reactivate the enzyme, AMPK, to the level that you need to say, bring down sugar levels for a diabetic. That's going to take either the drug Metformin or maybe even these plants extracts. Let's take a look at these two plant extracts that could be the new Metformins.
The first one is called gynostemma pentaphyllum and this was studied, as a matter of fact, this was studied several times, in cell culture studies, in clinical research with diabetics, with healthy people and I'm just going to go over one of the published research studies here. This had 24 Type 2 diabetics. Here's a study where they're actually using diabetics. Now, these 24 diabetics were not on any medications at this point.
Why? I don't know, but they weren't and they were given six grams of gynostemma pentaphyllum, which is a plant, and they were given it in a tea form. They compared this to green tea, which is known to help a little bit with diabetics--not tremendously, but a little bit. Green tea will improve insulin sensitivity a little bit, bring down sugar levels a little bit, so there is some benefit with green tea.
I thought this was interesting that they are taking this gynostemma pentaphyllum tea versus green tea in diabetics who aren't being treated. It was a twelve week study. That's a decent amount of time. The results of gynostemma pentaphyllum compared with green tea was this: there was a five-fold reduction in fasting glucose. The average drop in fasting glucose in the subjects drinking the gynostemma pentaphyllum was 54 points versus only 10 points for the green tea.
A fifty-four point drop. That's awesome. That's pretty close to what Metformin does, that's why I said is this the new a Metformin. There is a ten-fold reduction in hemoglobin A1C for the gynostemma pentaphyllum subjects. That's two percentage points versus only 0.2 percentage points of those taking green tea. So when you reduce hemoglobin A1C, that's your overall glycation burden coming down.
High levels of sugar will bind to proteins and that's called glycation, so we're bringing that down with gynostemma. And then, there was a near three-fold decrease in insulin resistance, which is the hallmark of Type 2 diabetes. This was published in Hormone and Metabolic Research, 2010. Gynostemma pentaphyllum activates AMPK and you're getting some tremendous blood sugar results from it.
The second extract is known as rose canina, also called dog rose. When dog rose blooms and flowers, it produces what is known as the rose hip, which I think more people are probably familiar with, but when you take some compounds from the stems and leaves of dog rose plants, the effects on blood sugar can be pretty tremendous.
Here, now, this was a mouse study, but we got to start somewhere and it was published in Journal of Pharmacology in 2011. They had some healthy mice and they had some diabetic mice and some of them were given the dog rose, some were given placebo. They looked at these mice for 15 days-- just 15 days--and the mice that were given, whether they were healthy or diabetic, if they were given dog rose extract, there was a significant reduction in blood glucose, a significant reduction in triglycerides, and a significant reduction in total cholesterol.
Why? Because you're managing sugar better by activating AMPK. So, gynostemma pentaphyllum and dog rose extract or rose canina, that's the plant. That combination activates AMPK and has some tremendous effects on blood sugar and very well could be the next Metformin.
Don't stop Metformin. Talk to your doctor about it, but there's some really good results here with natural plant extracts.
This is Healthy Talk on RadioMD.
I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

Listen in as Dr. Mike provides the answers to a wealth of health and wellness questions.
Additional Info
- Segment Number 5
- Audio File healthy_talk/1520ht4e.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 14, 2015
Host: Michael Smith, MD
RadioMD. It's time to ask Dr. Mike. Do you have a question about your health? Dr. Mike can answer your questions. Just email AskDrMikeSmith@RadioMD.com or call now 877-711-5211. The lines are open.
MIKE: Two years ago I joined a live, medical on-line forum that WebMD did. It was on gastrointestinal disorders. An update on inflammatory bowel disease, cilia, and that kind of stuff.
I was just really listening and I wasn't really paying attention until another doctor asked the question, "What is leaky gut?" That caught my attention because you have to remember, I have been working in the natural medicine industry for about ten years now, so I think I am a little more familiar with leaky gut that most medical doctors. Naturopathic doctors, chiropractors--they are much more up to date on this concept of leaky gut than an average M.D., but I am better than the average M.D. When I saw that question asked, it caught my attention and I was really curious to see how the moderator for this forum was going to answer the question.
His answer was something along the lines of "Leaky gut means you still have a diagnosis that needs to be diagnosed, or you still have a disease that needs to be diagnosed." It was his way of skirting having to answer the question because he probably really didn't know. That is how a lot of medical doctors see this idea of leaky gut. It's not something that we are really taught in medicine. Although we are a little bit and I'll explain that in a moment. Leaky gut is one of those things where, to a medical doctor, they just need to do a better job at figuring out what the actual disease is.
That is how most medical doctors see this concept of leaky gut. In answering the question, I think we first have to just give a clear cut definition of what leaky gut is. All it is, is hyperpermeability of the gut lining. Obviously, when you bring things into your GI tract--it is a tube for the most part--it digests all of these foods and it brings in the stuff you want and it keeps out the stuff you don't want. There is a very specific type of permeability between the lumen of the gut and bringing stuff into the bloodstream. It is permeable, things do get in, but it is selective.
The gut is a smart tube. It's not just a tube, it's a smart tube. It's permeable, but it's selective in what it allows to permeate into your bloodstream. It has to be. You don't want to bring in toxins and poisons.
It is not a perfect thing. It's not a genius at this, but it is smart. It does keep bad things out, but even in a healthy gut, obviously, toxins and stuff gets in, but that's where you get the liver to detox stuff. But that's the role of the gut, to bring in the stuff that you want, leave out the stuff that you don't want and then that stuff you don't want goes out the other end. That's a pretty simple way to think about it.
Leaky gut is when too much of the stuff that you don't want gets in. It becomes hyper, a high level of permeability to things normally that would have been kept out; now get into your system. That is leaky gut-hyper permeability.
The question becomes – why, then? When that happens, symptoms of leaky gut could be a lot of body aches, muscle aches, joint aches, pain syndromes, are very common in leaky gut. Because inflammation goes up, for instance, more toxins are getting in. That is probably the link. Bloating, gas, all of these things. You could have a lot of digestive symptoms, but you can also have more systemic type symptoms. Food sensitivities go up with leaky gut. Stuff like that. The question is what is causing it.
In one respect, the M.D.s like my colleagues were right. In many cases, there is a reason for it and that should be investigated. For instance, we know that in the context of hyperpermeability, leaky gut, there is a higher risk for inflammatory bowel disease, irritable bowel disease, celiac disease. There needs to be an appropriate work up. If somebody comes in with aches and pains and bloating and gas there are some very basic things that any doctor should do.
Digestive enzymes and a good work up of the bowel itself. Maybe even a scope looking at the lining. Is there some inflammation there that might be causing that? Because you want to rule out some of those major diagnoses. Of course, we don't really know if something like inflammatory bowel disease, like Crone's disease, is causing the hyperpermeability or the hyperpermeability caused the Crone's disease.
That is still a question, we're not really sure which way it goes, but there does need to be a good work up. But once you've ruled out those big diagnoses, the irritable bowel, inflammatory bowel, celiac, ulcer disease, once you've ruled a lot of that stuff out, you are left with just this unknown reason for somebody to have these symptoms that seem to be hyperpermeability. This is where I think medical doctors do a big disservice to patients. Often we don't know what to do at that point.
We don't offer a lot. This is where natural medicine really shines in these kinds of cases. What is leaky gut? It's hyperpermeability. It is caused often by some of these bigger bowel diagnoses. You have to rule those out. If you rule those out and you still have the symptoms of hyperpermeability, here are some things that you can do. Carnosine.
It is a dipeptide of alanine and histidine. Carnosine is very soothing to the gut; it has a healing property to the gut.
About a thousand milligrams a day. There is an herb called picrorhiza. I can never remember if it is a Himalayan herb or an Amazonian herb. I always forget where picrorhiza is naturally from. Picrorhiza is an herb that also has some of those same properties of carnosine. At Life Extension, we have been using picrorhiza for a few years now based on some good, good research in ulcer disease. Licorice extract – also good for the gut lining. Zinc is also very important.
As a matter of fact, there is this complex of zinc and carnosine that the Japanese have been using as a prescription drug for a long time to heal ulcers. If we need to heal the gut, if we need to decrease the inflammation and allow repair and healing to occur so we can decrease the permeability, maybe that zinc/carnosine combination that they use in Japan for ulcers might be appropriate here.
So, there are some things that you can do. Of course, you are going to want to detox as well, because with leaky gut, with hyperpermeability, you're brining a lot of gunk that you don't want. So, it's important to raise antioxidants in your body. It's important to do some liver support products like milk thistle and artichoke extract, and B vitamins and glutathione. Those are all critical to all the different stages or phases of detoxification in the liver.
Support your liver as well. Also, some anti-inflammatories. Your fish oils, your tart cherry extracts, the curcumin, all of those can be done. Boswellia extract—a medicinal plant—is one of my favorites for an anti-inflammatory regimen.
So, what is leaky gut? In very simple terms, it's just things that you don't want to get into your system get in because the gut has lost its ability to be selective in what it allows to permeate in, so it is hyperpermeability. Carnosine, picrorhiza, licorice, zinc, do some detox--those things are going to help with leaky gut.
But make sure you rule out a big diagnosis. This is Healthy Talk on RadioMD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD
Listen in as Dr. Mike provides the answers to a wealth of health and wellness questions.
Additional Info
- Segment Number 4
- Audio File healthy_talk/1520ht4d.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 14, 2015
Host: Michael Smith, MD
You're listening to RadioMD. It's time to ask Dr. Mike on Healthy Talk. Call or email to ask your questions now. Email AskDrMikeSmith@RadioMD.com or call 887-711-5211. The lines are open.
DR. MIKE: So, answering the first question that I have today, I could do a whole hour show on this. I could do a whole week's worth of shows on this. It is just so important. I am going to do my best to answer this question and be thorough about it. The question is simple.
"How important is magnesium to a diabetes protocol?"
The simple answer, and we could just end right here, would be—very. That's it. Take magnesium. But I want to get into some of the science a little bit.
I'm going to look back and present to my listeners a study in 2003 in Diabetes Care. It was one of the first studies that really looked at magnesium and a lot of the diabetic measurements that we look at as doctors and the improvements there. And there was just a recent one late last year that came out, also showing and kind of confirming, that earlier study.
Let's not forget something, magnesium is critical. It is involved--it depends on who you read on this. Some people claim, some physiologists claim. that it is involved with over a thousand metabolic reactions in the body, some say 350. Whatever. Magnesium is critical. It is critical for highly metabolic, electrochemical cells—meaning nerve cells, brain cells, muscle cells. Which, obviously, means your heart, gut--your gut cells are highly metabolically active.
All of those types of cells that are constantly turning over. Contracting, firing electrical impulses. Digesting food. Cells that need a lot of energy that have to manage energy well. They all require lots and lots of magnesium.
When you look at a lot of the age-related disorders that we deal with today—diabetes, neuromuscular problems, brain disorders, heart disease, even cancers—when you look at all of them. there is an interesting correlation. As we have confirmed now through the U.S.D.A.--starting probably in the 70s or 80s--there was a sharp drop in Americans who had adequate magnesium levels. There was a sharp drop and that has been sustained through the 70s, 80s, and 90s. We are as a country, and I am just speaking about the United States right now.
We, as a country, have a populous that it's an epidemic. We are deficient in magnesium. There are different theories as to why this is. For me, it's pretty simple. It goes back to soil conditions. The soils in the United States haven't been very healthy for many decades now and when you have unhealthy soils, you lose the ability of the soils to hold onto the minerals. They get leeched very easy with just one rain storm. We have soil conditions that are mineral deficient, including magnesium, which means the food sources are mineral depleted, included magnesium. To me, it goes back to just growing, and cultivating, and farming healthy food from healthy soil.
That to me is the main reason. We are low in magnesium and there is this nice correlation with blood pressure, heart disease, cancers. You have to be careful, it's not cause-effect, and I'm not saying that. But there is definitely this relation between loss of magnesium and age-related disorders.
We know, by the way, if you give people magnesium, they do better in a lot of these conditions. It doesn't always necessarily treat the condition, but some of the things we look at as doctors, improve. Let's go right to the question—how important is magnesium to a diabetes protocol? As I said--very. Let me just show you this. If you improve magnesium levels in a diabetic or a pre-diabetic or somebody at risk for diabetes, all of the things we look at--blood sugar, hemoglobin A1C, insulin resistance—all of these things improve when you improve, or even just correct, the magnesium deficiency.
\This first study was published in Diabetes Care in 2003. This was a study that was looking to determine whether oral magnesium supplement improves both insulin sensitivity and metabolic control in Type 2 diabetes subjects with decreased serum magnesium levels. They found Type 2 diabetics with low magnesium, that's who was brought into this study.
This was a randomized, double-blind, placebo-controlled trial of 63 subjects who had Type 2 diabetes, decreased serum magnesium levels and they were on a sulfonylurea. Back in the early 2000s, that's pretty much what we used. Metformin was around, but it was not as popular as it is today. They were all on a classic sulfonylurea to treat diabetes, called glynase. It is not really used that much anymore today. They had 63 diabetics on a very common drug back then, and they all had low magnesium levels.
They then split the groups up. Half of them received a solution of magnesium chloride and the other half, a placebo for 16 weeks. Not only did they look at all of the basic things like blood sugar level, hemoglobin, they also did a very standard measurement model for insulin resistance called HOMAIR.
It stands for homeostasis model assessment for insulin resistance--a very classic model for measuring insulin sensitivity. The results were clear cut. "At the end of the study, the subjects who received magnesium supplementation showed significantly higher serum mutation concentration." You would expect that. Their magnesium levels went up. They took the magnesium solution and their magnesium levels went up. That's the first thing that they had to make sure was happening.
So, the magnesium levels improved by those taking the solution. The placebo group--the magnesium levels stayed low. As magnesium levels went up in this study, there was an improvement in the insulin resistance measurement. There was a significant improvement—all of these results were significant, meaning statistically significant—there was an improvement in insulin resistance, fasting glucose level and hemoglobin A-1C. Everything improved across the board significantly and the only difference was improving magnesium levels. Awesome. Magnesium didn't become a standard treatment for diabetics at that point.
In 2003, we still—I was a young practicing physician at that point—we weren't talking about magnesium. You have to ask the question—why? What's going on? The argument would be--just 63 people, it was a small study. It's interesting, it is hypothesis generating, blah, blah, blah. At some point we've got to start taking what we're finding in clinical research and start applying that to everyday practice.
We have to start doing that quicker and sooner, especially with something as simple as magnesium. They conclude that "Oral supplementation with magnesium restores serum magnesium levels." Good. "It improves insulin sensitivity." Good. And "It improves metabolic control in Type 2 diabetics". That was the conclusion of a really well-designed, straight forward study.
You improve magnesium levels. All of these basic parameters we look at, the main ones. Insulin sensitivity, glucose levels, and hemoglobin all approved across the board. This most recent one was published in the Journal of Human Nutrition and Food Science and it basically just did the same thing.
It was a review. Since 2003, there have been repeated studies of this one in Diabetes Care. Several of them, actually. They went back and looked at those. They went back and looked at all of those similar studies from 2003 up until the current date and they all have the same conclusions. Low magnesium is bad for diabetics and improving magnesium levels, giving people magnesium, improves all the parameters we look at in a diabetic.
So, if you're diabetic, pre-diabetic or you are at risk, you have to be taking at least 500 milligrams of magnesium every day.
This is Healthy Talk on RadioMD.
I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

How can you lose weight without feeling hungry all the time?
Additional Info
- Segment Number 3
- Audio File healthy_talk/1520ht4c.mp3
- Featured Speaker Eddie Fatakhov, MD
- Book Title The Doctors’ Clinic-30 Program
- Guest Website Eddie Fatakhov
-
Guest Bio
 Eddie Fatakhov, M.D., M.B.A., has spent years as a personal trainer and nutritionist, helping his clients with weight issues and providing them with tools for a healthier lifestyle. He is also author of the Doctors' Clinic 30 Program.
Eddie Fatakhov, M.D., M.B.A., has spent years as a personal trainer and nutritionist, helping his clients with weight issues and providing them with tools for a healthier lifestyle. He is also author of the Doctors' Clinic 30 Program.
Now, as a physician in training and a member of American Society of Bariatric Physicians, he plans to dedicate his focus on bariatric medicine (weight loss management specialist) to help his patients not only lose weight, but to keep it off. -
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 14, 2015
Host: Michael Smith, MD
Healthy Talk with Dr. Michael Smith, M.D. And now here's the country doctor with a city education, Dr. Mike.
DR. MIKE: My guest is Dr. Eddie Fatakov. He came from Russia to the United States and eventually made it down to the south. He dealt with some pre-teen and teen weight issues himself and has really dedicated his medical career now to not just really the weight loss part of it, but keeping it off and that healthier lifestyle.
Dr. Fatakov, welcome to Healthy Talk.
DR. FATAKOV: Thanks for having me, Dr. Mike. Glad to be here.
DR. MIKE: I went on your website. My listeners, I want you guys to go and check him out. It's www.drfatakhov.com. The book is there, the Doctor's Clinic Thirty Program and you can read a little bit about Dr. Fatakhov. We were just talking about the importance of the question "Why I am gaining weight in the first place". What do you think about that question? How important is that Dr. Fatakhov?
DR. FATAKOV: I think it is the most important question. That is the question asked by most people who come into my office. The important question is how many meals a day are you eating and are you eating breakfast? If that is the answer, that's where I start. Most of my patients—90% -- I get them to eat six meals a day and eat breakfast and drink water and get a good night's rest and then they have no troubles losing weight. It is changing habits.
A diet is temporary. We diet for reasons: for spring break, to get ready for a wedding, to lower our blood pressure, if we're on diabetic diet, to get our sugars under control. It's already pre-programmed that it's going to be temporary, it's never lifelong. If we develop good habits as a child—and there have been studies on this--they develop good habits and are going to eat healthy if their parents eat healthy. They will eat healthy the rest of their life and they will be healthy. Is it genetics or environmental? It's a little bit of both.
DR. MIKE: Besides this eating pattern, like you call a sumo wrestle, ultimately it's just pigging out at the end of the day, alcohol added in there, going to bed, not active enough. That type of pattern. Other than that, though, what are some of the other reasons you think we have such a weight issue in this country?
DR. FATAKOV: It's overindulgence and the fact that we are lucky we live in a country where food is accessible. Processed food, refined carbohydrates and there are a lot of chemicals in stuff like that and then the high fat content. They have done studies where you can eat low fat or low carb but these sugars, these simple sugars, are basically making us obese and preventing fat breakdown. They are the biggest reasons.
Then, you have the high fructose corn syrup which gets processed like sugar. Somebody eating these meals, it's no different then eating a Snickers bar. You think you're eating healthy, but you're not. And it is misleading. You go out to the grocery store and there are 50 multi-grain bread—all it is is white bread with 50 grains in it. It's not 100% whole wheat. It is just education. I think the public is not educated because there is so much information out there.
You don't know what is good or what's not. The Mediterranean diet is great, which adds lot of fat and a lot of olive oil. Healthy is different from weight loss, but people don't get that. But too much of a good thing is a bad thing.
DR. MIKE: I had Dr. Stephen Sinatra on my show once, Dr. Fatakov. He is one of the premiere cardiologists in the country, in my opinion, and he links a lot of our issues back to the 80s where fat became the culprit in all of this.
So, we got rid of the fat but then we added all this sugar. Now, we have worse heart disease and more overweight people and we are finally starting to get it that those simple sugars, those simple carbs—those are the things we need to control. Let's talk about this losing weight without feeling hungry. That is an issue. People start dieting, they start cutting calories a little bit—even on your program. Let's say they are eating their six smaller meals, but now an hour or two hours later they have all of this hunger. How do we help them control that?
DR. FATAKOV: In terms of the hunger urges, you have multiple reasons. You have the escalated hormone levels. What I tell my patients to do is that you don't want to restrict it. The word diet fails. There did a study in Psychology a few months ago. 83% of those who use the word diet, those patients fail. It is more of a program and a lifestyle. The way I designed the book is a slim phase and a maintain phase and an education phase. So, you use slim to get to your goal weight. You use the maintain phase to stay where you are at, in addition to exercise and good eating habits.
The way you do that is eating more to lose more. I provide plenty of food options. I want to be honest, nobody really likes to diet. Nobody wants to be on a diet. Nobody really cares to diet. People just want to get results and the easiest way to do that. It's not about restriction. I never want to restrict. I always want them to eat more to lose more. A perfect example, I'm giving one of my patients. She said, "I want chips and my doctor said I can't have chips." Well as soon as you say "no", she's going to get chips whether you tell her she can have them or not.
I asked, "When are you eating chips?" She said, "In my living room when I watch TV." I said, "How far is the kitchen?" The kitchen is a walk. I told her to put the chips in the kitchen, each time a commercial break comes on she will go grab one chip, chew it and come back and sit down.
How many times do you think she is going to get up out of her favorite chair to go get chips? Now, I never said "no". Right now, if I say, "You can't have a cookie. You didn't want a cookie until I mentioned it." The whole way of thinking is now, "I want a cookie", just because I said "no". We can't take no. If you want Chic-Fil-A on Sundays, you can't have it on Sundays. It's just psychologically built in.
I never say "no" to any of my patients. I say if you're going to have your worse meal, have it at breakfast. You have the whole day to burn it. If you are going to eat bad, have it at breakfast. The food table contains plenty of fruit and vegetables and stuff like that they can have--unlimited foods. My plan is based on extensive research that has been out for several years. It's proven. That's why Weight Watchers has been so successful because it doesn't restrict people on what they can and cannot eat.
DR. MIKE: In some of your experience, what are some of the common roadblocks that people face? They are eating more. They are eating less. They are being more active. They are having some success. At that point, what are some of the things you like to warn people to watch out for so they don't backtrack on their weight loss plan?
DR. FATAKOV: You get this plateau. The first month they are motivated, they are seeing results. Then they get depressed, "I'm not losing as much weight. Once you get to that point, there might be a four week or six week plateau, then we ramp it up. We change something in their diet. We tweak things around. That's when people don't get motivated to work hard to maintain stamina. That's when we encourage them to eat better and get more exercise. Sometimes people exercise and are gaining muscle and when they look on the scale, they have the same weight.
They are not losing weight. I always make them do leg circumference and arm circumference and the inches keep dropping. So, it's just the training and counseling. When they come to the doctor's office, see a nutritionist or a personal trainer, it creates accountability. People say, "When I go to my doctor, I'm going to make sure my blood pressure is normal," and "When I go to my doctor, I want to make sure I'm not gaining weight." So, if you have that personal accountability, it reinforces it.
DR. MIKE: I have a little theory. Let me run this by you, Dr. Fatakov. See what you think about this. This is just my own little theory, my own little experience helping people lose weight. Everybody has certain flavors and textures that they enjoy. If you eliminate those, if you take those away, no matter what diet program you are on, if you take away, those flavors and textures that people enjoy that is really going to make the cheating kick in. It's going to make it hard. How important do you think it is to recognize the things that you like and try to figure out healthy alternatives so you get those same flavors and same textures? Am I on to something there?
DR. FATAKOV: You are on to something. People love bacon, right? They just love bacon, even if it's turkey bacon. If you fry eggplant – deep fried eggplant – it tastes just like bacon. It's more about the texture, just like you're saying. There are people here from different ethnicities. Some are Indian, some are from the Carribbean, some are from Russia like myself. If you go to a doctor or dietician and they say you can only have this or this and it's not culturally diverse enough or doesn't have the same texture that you're used to—you are going to cheat. I think you are on to something. That is very important. That's why having that fried eggplant tasting like bacon and being as crisp is just as important, mentally.
DR. MIKE: I had a guest on that talked about the importance of maybe having one meal on occasion where you do cheat a little bit. Not overdoing it, not overeating. You have that bacon once in a while. How important do you think it is to allow people to cheat once in a while? Is that going to be helpful in them sticking with that diet?
DR. FATAKOV: Now that's very interesting. I'm on both sides about this. They just came out with an interesting study in the Journal of Obesity. It said having one fat meal will alter your metabolism for muscle storage and muscle building for up to five days. And it could take up to two weeks to get it back into the cycle. I think having that one meal can set you back for a long time with all the hard work that paid off. Until you get to the goal weight, where you are happy at the weight, I wouldn't cheat.
DR. MIKE: You wouldn't cheat. Maybe a little bit down the line, when you are just trying to maintain, that cheat meal is okay. His name is Dr. Eddie Fatakov. You can check him out at www.drfatakov.com and I appreciate you coming on. Great job and continue your great work.
This is Healthy Talk on RadioMD.
I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD

How is eating like a toddler different from how adults eat?
Additional Info
- Segment Number 2
- Audio File healthy_talk/1520ht4b.mp3
- Featured Speaker Eddie Fatakhov, MD
- Book Title The Doctors’ Clinic-30 Program
- Guest Website Eddie Fatakhov
-
Guest Bio
Eddie Fatakhov, M.D., M.B.A., has spent years as a personal trainer and nutritionist, helping his clients with weight issues and providing them with tools for a healthier lifestyle. He is also author of the Doctors' Clinic 30 Program.
Now, as a physician in training and a member of American Society of Bariatric Physicians, he plans to dedicate his focus on bariatric medicine (weight loss management specialist) to help his patients not only lose weight, but to keep it off. -
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 14, 2015
Host: Michael Smith, MD
Anti-aging and disease prevention radio is right here on Radio MD. Here's author, blogger, lecturer and national medical media personality, Dr. Michael Smith, MD with Healthy Talk.
DR MIKE: So, what do I mean, eating like a baby can help with weight loss? My guest is Dr. Eddie Fatakhov. He was first, I think, a personal trainer, a nutritionist and he spent a lot of time helping clients with weight issues, healthier lifestyles. He even authored a program or book called Doctor's Clinic 30-Minute Program. And now he's a physician. I think he's in his residency, if I'm not mistaken. He's a member of the American Society of Geriatric Physicians. He plans to dedicate his focus on weight loss management to help his patients not only lose weight but to keep it off.
Dr. Fatakhov, welcome to Healthy Talk.
DR FATAKHOV: Thank you so much for inviting me, Dr. Mike.
DR MIKE: So, how did you know, being a young physician, how did you know you wanted to focus on weight issues?
DR FATAKHOV: Well, ever since a young age, I was overweight myself as a preteen and teen. Actually, I moved from Russia to New York. So, you never have to take your shirt off because it's cold. So, when I moved down to the south down here in Atlanta, George, and, you know, just going to the pool and being around everybody I just kind of became self-conscious and it wasn't until I broke my arm and went into rehab that I started going to the gym, working out and playing sports, I became an advocate about it and I became self-confident about myself. And a big part of my life as a personal trainer, as nutritionist as a dietician major, now, as a physician and an obesity specialist, so that's something I'm passionate about.
DR MIKE: Yes That's awesome. And I was familiar with your story a little bit because my producer Sheldon Baker sent me your bio. I like it when practitioners, doctors, trainers, whatever, have kind of like that personal connection to the specialty that they are going in. That adds a lot of passion and motivation to it. So, great job there. What do we mean or what do you mean eating like a baby helps weight loss? Maybe we need just to start there. What does that mean to eat like a baby?
DR FATAKHOV: So, basically, it's the pattern or behaviors that's like a baby. People come in to my weight loss clinic and all of them, and you've probably heard this. You've probably done this with some of your patients. They come and they say...I'm like, "What do you eat?" I ask two questions to everybody before I get [inaudible 02:35] "How many meals do you eat? Do you eat six meals times a day and do you eat breakfast?" More than 90% say "no".
And so, I pose a question to them. So I say, "You're pretty much eating like a sumo wrestler." And then they're baffled. "Oh, my god." And then I say, "Sumo wrestlers eat one or two meals a day. They skip breakfast, they fast when they work out.
They binge eat at night, they go to sleep. They go out to drink beer and alcohol like most Americans do. Go out to restaurants and when they thought about that and so they're eating to gain weight and you're coming here eating like a sumo wrestler expecting to lose weight. And that's why I make the conditions. She said, "Well, I'm a sumo wrestler, doctor. What do I need to eat? How should I eat like? And I said, "You need to eat like a toddler?" And that's where the concept kind of...why I started on the concept.
DR MIKE: So, explain then what is the eating pattern of a toddler?
DR FATAKHOV: Okay, so a toddler has a natural rhythm. They're born with it. The first day, their stomach size is small, size of a grape, size of a walnut by the second day. By the tenth day it goes to large grapefruit and then adult stomach is about the size of a big softball. So, they can't eat big portions. They eat small portions. So, what I tell my patients is, toddlers never skip breakfast. And they've done studies in 2010 in that people who don't eat breakfast tend to be overweight and obese versus their counterparts. So, I said, "Toddlers never skip breakfast like the 36 million Americans do." There was a recent Huffington Post article on that. So, it's the pattern of a toddler. They eat six meals a day. They've done studies on blood sugar control and metabolism and we lose more if we eat more frequently, so, you know...
DR MIKE: Yes. So, I would--just backing up to that so, going back to that concept of the small stomach. So, they have a small stomach, they can only eat so much anyway. They can only get so many calories in there before it extends and they feel full, requiring them to have another meal, maybe two or three hours later. So, what we're trying to do is re-train the adult stomach to kind of act that way and we do that by these smaller meals. That's basically the theory, right?
DR FATAKHOV: Exactly. So, eat the small meals and it stabilizes the blood sugar which prevents a lot of insulin release; prevents fat [inaudible 04:40] promotes fat burning by re-programming the metabolism.
DR MIKE: Now, that's an interesting concept because I even did some of my own research, Dr. Fatakhov, on the link between insulin sensitivity issues and weight gain. We know that when people are insulin insensitive, I'm not going to call it insulin resistant because that's Type 2 Diabetes but we can - it's kind of a spectrum of levels of insulin sensitivity The worse that gets, the harder it becomes to manage sugar, the harder the cell has a time in burning sugar versus storing it as fat. And what you're saying, if we go back to eating like a toddler that alone also helps in insulin sensitivity. Correct?
DR FATAKHOV: Correct. And if we look at what toddlers eat, they actually have a pretty good ratio of fats and carbohydrates. They eat a well-balanced meal and so another reason is they eat healthy. There's no mother I know that won't cook good, organic food, natural food, spend hours cooking for their toddler.
So, mothers and family members make sure the child gets the best nutritious food and the healthiest food so that they can have proper food. We don't do that as Americans and the last time I checked, toddlers don't go to Burger King and eat. They don't go out and get drunk as their adult counterparts. So, just having the behaviors of a toddler promotes a healthy lifestyle.
DR MIKE: So, working. I've been in corporate America now, Dr. Fatakhov, for maybe twelve years and I see that very pattern. I have colleagues that I know they rush in, they've had their Starbucks coffee or latte or - there's usually some sort of whipped cream on top of it. So, they got their sugar load, their caffeine load. They work pretty much through lunch, maybe at lunch they have a small something, whatever. They're starving by the time they go home. They go to a restaurant, they pig out, they have three or four drinks and then they go home and go to bed. That's a pretty typical day for a lot of my colleagues and that is completely the opposite of a kid, right?
DR FATAKHOV: Exactly. That's more of a pattern of a sumo wrestler. And they probably aware and they've done studies where if you go out to eat with your colleagues, 40% more fat you consume. 30% more calories consume because we are socializing and don't think about it. Plus, at the restaurant, you don't know how many calories there are preparing the food versus at home when you're mother or father and you're preparing the food for this individual. You know exactly what you're putting into his body.
DR MIKE: So, how do we do this then? How do we help somebody? Help an adult break this pattern that I just described which we both know is very - and my listeners know it – it's a very common scenario of that type of pattern of eating, gorging yourself, usually in the evening. How do we break that? We can't just tell patients and friends and family, "Well, don't do that. You got to eat six meals a day." Do you have like a step-up program that you put people on? What is the best way to get someone to break that pattern?
DR FATAKHOV: Yes, with my patients it's hard because they're 60 years old, some of them are 70, and they've been eating like that for twenty, thirty years so hard to convince them eat six meals all of a sudden. So, I say, let's just say you eat breakfast or you might eat dinner and what I try to do is I'd incorporate snacks in there. That's what I do. People can snack on something that's healthy.
Let's fill in one snack. Let's do 4 meals for this week and I'll keep them at 4 meals because anything is better than the one or two meals because you don't want to have your biggest meal ...70% of your meal every day should be throughout the day and maybe 20-30% at night. But it's the opposite. You're having 70% of all you're calories at night. When you come home from work, when you're relaxing in front of the TV and 30% is throughout the day. Now, we have to change it up a lot. [inaudible 08:19] a good pattern. You know?
DR MIKE: Yes. What I like about your system here,
Dr. Fatakhov, is I think sometimes in the weight loss industry we ask the wrong question. So often people will ask, "How do I lose weight? What's the best diet for me to go on to drop the pound, shed the weight, etc. etc.?" When really maybe the better question is why we're gaining the weight in the first place? Right?
DR FATAKHOV: Exactly.
DR MIKE: And we know that there are physiological reasons for that. We just talked about insulin sensitivity. There is hormone issues. There's a lot of reasons there but what you've identified is an eating pattern that might be driving that weight gain. So, maybe the first thing we do is we got to correct that underlining problem and then when they do try, maybe they want to eat more protein, less carbs, whatever. That's fine. That might have a better chance of working. Correct?
DR FATAKHOV: Correct. You actually hit the nail on the head. [inaudible 9:12]
DR MIKE: I'll tell you what, Dr. Fatakhov, let's hold that thought. We'll come back to that. We, also in the next segment will get into losing weight without feeling hungry.
I'm here with Dr. Eddie Fatakhov and we'll continue our discussion in a moment.
This is Healthy Talk on Radio MD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD
If you have excess homocysteine, you might be at an elevated risk for heart disease, stroke, and other health issues.
Additional Info
- Segment Number 1
- Audio File healthy_talk/1520ht4a.mp3
- Featured Speaker Mike Smith, MD
- Organization Life Extension
- Guest Website Healthy Talk MD
-
Transcription
RadioMD Presents: Healthy Talk | Original Air Date: May 14, 2015
Host: Michael Smith, MD
Healthy Talk with Dr. Michael Smith, M.D. And now here's the country doctor with a city education, Dr. Mike.
DR MIKE: So, I want to talk about homocysteine. Specifically, I want to talk about some newly identified risks of having too much homocysteine in your body. I think in the medical community most doctors accept now homocysteine or high levels of homocysteine as a risk factor for heart disease.
But new research is showing that it can also impact dementia, Alzheimer's and diabetes--believe it or not. I want to talk about that. The first thing that I think we need to do is just talk about what is homocysteine? And, why is it so damaging to the body?
When you eat dietary protein—proteins are made of building blocks called amino acids—when you eat chicken or whatever protein source, you digest the protein. Essentially, you release the amino acids that make up that protein. They get into your blood stream. One of those amino acids is called methionine. Methionine has a lot of roles in the body itself. It is an important amino acid in DNA protection and muscle production.
Methionine will, inside of the cell, convert into homocysteine. Homocysteine is really just this intermediate amino acid because when you have vitamin B6 on board, homocysteine becomes cysteine. And cysteine is an important amino acid for all kinds of stuff, too. In particular, cysteine will convert eventually down to glutathione, which is the most important antioxidant for your body.
That is kind of the pathway that we like to see when you eat protein. Methionine to homocysteine with vitamin B6. It turns into cysteine and then eventually glutathione. That is a very important pathway. However, if you don't have enough vitamin B6 on board, homocysteine cannot turn into cysteine and that pathway breaks down and homocysteine actually builds up. There is one little side pathway that can happen. Homocysteine can convert back into methionine with vitamin B12. So, vitamin B12 and vitamin B6 are critical to maintaining healthy levels of homocysteine in your body.
But you might ask, "Okay, Dr. Mike, what is the big deal? So what if homocysteine actually builds up? What's the big deal?" There is some evidence, and I presented this to a group of cardiologist a couple of years ago here in south Florida, showing how homocysteine damages what are called "adhesion molecules" that hold together the endothelial lining. That is the inside lining of the arteries.
So, there is some evidence out there that homocysteine is a direct insult—causes a direct damage—to the inside lining of arteries. That includes your heart and your brain and so forth. We want to keep homocysteine levels in a nice optimal range, usually less than about five. That is going to be a nice optimal range if you do check homocysteine on a blood test, which you can. B6 and B12 are critical to keeping that down. A high level of homocysteine is considered a cardiovascular disease risk factor, but there are some other problems with high levels of homocysteine. It is also implicated in vascular dementia.
That is a form of dementia, not Alzheimer's dementia. There are different kinds of dementia. Vascular dementia is usually where you just have repeated small strokes and homocysteine seems to play a role in that.
In a study published in 2014, 64 people with vascular cognitive impairment—like mini strokes—but they didn't really have dementia, they were studied. After only one year, patients with high homocysteine in that group showed a 4.2 fold increase rate of getting dementia down the line. Here you have a group of patients with multiple little strokes and you can actually see that on a CAT scan.
They are able to do all of the cognitive tests, so they don't have dementia yet, but if homocysteine creeps up, there is a 4.2 increase risk of developing a vascular dementia down the line. As a matter of fact, the authors of that study said "Patients with vascular cognitive impairment should receive vigorous controls of high homocysteine level." The journal that came from, this was a Chinese study, I cannot pronounce the journal.
It was a peer-reviewed Chinese journal from 2014. In another 2014 study, they looked at people with high homocysteine in uric acid and find a startling 10.5 fold greater risk for vascular dementia. So, when homocysteine is high and uric acid are high, you're talking about a 10.5 increase risk of vascular dementia. That's huge.
These are the types of numbers that we can't allow conventional doctors to just ignore. That is just amazing that homocysteine, and, in this case, coupled with uric acid, can increase vascular dementia risk that much. That came from the Journal of Neurological Science, 2014. There are many other studies that actually show that link between high homocysteine and vascular dementia. There was a 2013 study that found patients with vascular dementia exhibited particularly elevated levels of plasma total homocysteine. Just confirming some of these other studies.
As a matter of fact, if you go to one of my favorite sites—I've talked about it before—PubMed.com has all of the research studies you want. You can just type in different search terms. You don't have to be a doctor to do all this. If you enter "homocysteine and vascular dementia" you'll pull up 240 published studies dating all the way back to 1992. There is a lot of credible evidence linking excess homocysteine to vascular dementia, not just heart disease. Another type of dementia is, of course, Alzheimer's dementia.
One theory is that what happens in Alzheimer's dementia is capillary blood flow—capillaries are the smaller vessels that actually feed into the tissues—that blood flow is impaired as a result of damage to the inside lining, the endothelial lining, and that is caused by excess homocysteine.
Remember, I mentioned before—homocysteine can directly damage those cells, those adhesion molecules that hold those endothelial cells together.Once that you have that kind of damage, beta amyloid plaques appear in these blood flow deprived areas of the brain because the capillaries just aren't working. They are kind of leaking.
The result, in many cases, is clinically diagnosed Alzheimer's disease. There was a really nice review of this in the British Medical Journal of Public Health, 2014. This was a systematic review of published studies starting in 1990 and extending to 2012 and they found that high homocysteine increased Alzheimer's risk by almost two-fold, whereas, physical activity and Omega3 fatty acids had a protective effect. That is homocysteine and Alzheimer's disease.
A 2013 review looked at the effects of lowering homocysteine for the purpose of protecting against mild cognitive impairment and Alzheimer's disease based on findings from several previous studies. These researchers concluded that "Treating patients with B vitamins could delay or prevent cognitive decline and Alzheimer's disease". Now, I'm not saying B vitamins are a treatment for Alzheimer's. Alzheimer's has many causes. It is multi-factorial. I did a whole review of that on my show once.
But, it looks like I need to add to that there could be an issue with high homocysteine in Alzheimer's patients and B vitamins could play a role in offering some protection. This one was interesting to me: Homocysteine can make diabetic complications worse. This was some new information from the C.D.C. "Eighty-six million Americans suffer from pre-diabetes." That is kind of a blood sugar level 102-125 milligrams per deciliter. It is not quite full blown diabetes yet.
What they found is if you fall in that range and you have high homocysteine, you are at a significant increase risk for developing full-blown diabetes down the line. So, lowering homocysteine is very important to somebody with pre-diabetes. Maybe just B6 and B12 would be a good way to protect from full-blown diabetes.
Get your homocysteine levels checked, make sure it is less than 5. If not, get on some B vitamins. Pretty simple.
This is Healthy Talk on RadioMD. I'm Dr. Mike. Stay well. - Length (mins) 10
- Waiver Received No
- Host Mike Smith, MD